In most cases, fibroids do not cause any symptoms and do not interfere with pregnancy and therefore no treatment is required.
In case of mild symptoms, the gynaecologist may consider no treatment but to monitor to see if they are growing.
Treatment is only warranted when the fibroids are large which interfere with pregnancy or fertility and cause symptoms.
The choice of treatment is highly individual and tailored to individual circumstances. There are important factors (see table) that you must consider and convey clearly to your gynaecologist so that in consultation you and him/her can agree on an appropriate treatment. They include questions below:
- Have you any symptoms?
- Do you want to become pregnant?
- Your age, e.g. are you near menopausal age?
- What is the size of the fibroid(s)
- Location of the fibroid(s) and how accessible the fibroids are.
In principles, a particular chosen treatment aims to achieve either [1] or [2], and in most cases (most women's wishes) both of the followings:
1. The management of abnormal uterine bleeding (AUB) which relieves symptoms of menorrhagia, anaemia, pelvic pressure effects (renal tract-urethra, bladder) and pelvic pain.
2. An attempt to improve fertility (reducing the risk of miscarriage).
Available treatment options for fibroids (Fig 1.) are summarised in the diagrams below and the choice is mainly governed by the woman's fertility wishes:
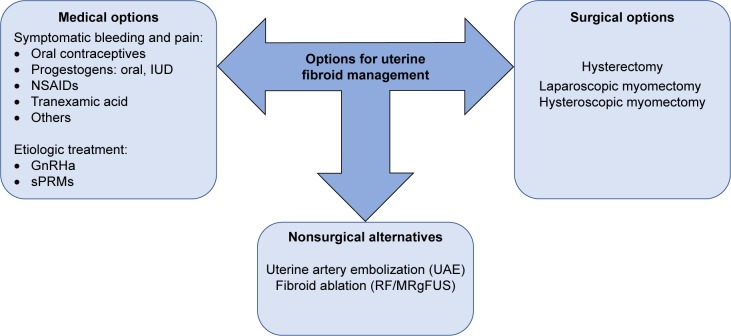
Fig.1 -Surgical, nonsurgical, and medical therapy currently used for the management of UFs.
Abbreviations: GnRHa, gonadotropin-releasing hormone agonists; IUD, intrauterine device; MRgFUS, magnetic resonance-guided focused ultrasound surgery; NSAIDs, nonsteroidal anti-inflammatory drugs; RF, radiofrequency ablation; sPRMs, selective progesterone receptor modulators; UAE, uterine artery embolization; UFs, uterine fibroids.
Fig 2. shows the typical flow diagram that guides appropriate choice of treatment of optimally meeting the patient's needs
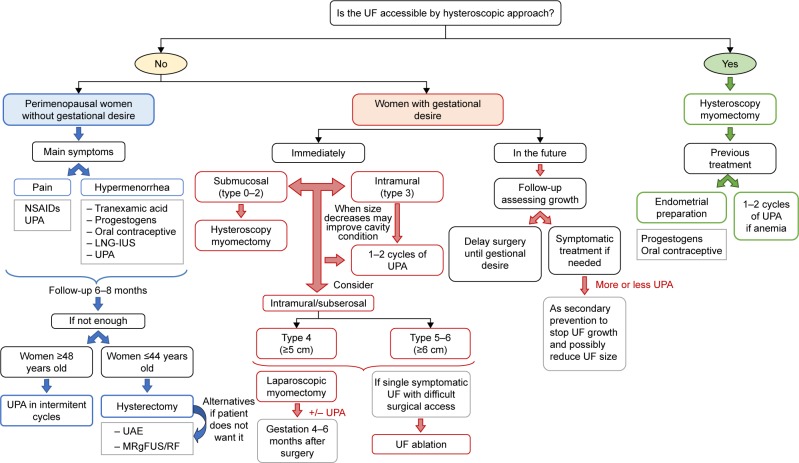
Fig.2 -Medical flowchart for the management of UFs according to the patient’s profile.
Abbreviations: LNG-IUS, levonorgestrel intrauterine system; MRgFUS, magnetic resonance-guided focused ultrasound surgery; NSAID, nonsteroidal anti-inflammatory drug; RF, radiofrequency ablation; UAE, uterine artery embolization; UF, uterine fibroid; UPA, ulipristal acetate.
| Table 1. Summary of available medical options | ||
| Group of medicines | Medicine name | Description |
| Drugs that reduce bleeding only. | Anti-inflammatory drugs | Known examples of this group of medicines are Ibuprofen and Mefenamic Acid.
These tablets reduce the production of natural substances in the body called prostaglandins, which are linked to heavy periods so bleeding becomes lighter. |
| Tranexamic Acid | It helps blood to clot in the womb (uterus) so bleeding becomes lighter. | |
| Combined oral contraceptives (COC) | They are sometimes called "the pill", which contain oestrogen and progestogen. Their hormonal actions slow down the growth of the uterus lining so bleeding becomes lighter. | |
| Levonorgestrel-releasing intrauterine system (LNG-IUS | A small plastic device that is inserted into the woman womb to slowly release a progestogen based hormone (levonorgestrel. This drug stops the lining of the uterus growing quickly so bleeding becomes lighter. | |
| Drugs that shrink the fibroids and reduce bleeding. | Ulipristal Acetate | A synthetic hormonal compound that prevents cells lining of uterus from multiplying and causes these cells to self-destruct. Consequently, ulipristal reduces the size of the fibroids and bleeding becomes lighter. |
| Gonadotropin releasing hormone analogues (GnRH agonists) | Commonly used products are injectable goserelin and triporelin.
They work by making the body to release a small amount of oestrogen which causes the fibroids to shrink and makes bleeding lighter. |
|
| Table 2. Summary of surgical and non-surgical proceedures for uterine fibroids | ||
| Type | Proceedure | Description |
| Non-Surgical | Endometrial Ablation | This involves removing the lining of the womb using energy source. The fibroids are not physically removed. The procedure causes the lining of the womb becoming unable to sustain the fibroid growth and bleeding becomes lighter or stopped. It is most suitable for fibroids that are located near the inner surface of the uterus. |
| Uterine Artery Embolisation (UAE) | This involves injecting small particles into the blood vessels that bring blood to the womb particularly those vessels feeding the fibroids becoming blocked. Without further blood supply, the fibroids could no longer grow and they eventually shrink. This technique is not suitable for every type of fibroids. | |
| Radio Frequency Ablation of Uterine Fibroids (RFAUF) | Under MRI guidance to locate the fibroids, heat energy is then applied through the needles to destroy them. Not all types of fibroids are suitable for this technique. | |
| Surgical | Myomectomy | This involves surgical removal of the fibroids; can be done via keyhole in some cases. It enables you to retain your womb and most suited when you still want to have children. This technique is not always possible because it depends on the size, number and location of the fibroids. |
| Hysterectomy | The womb is surgically removed; in most cases the ovaries are left behind to avoid pre-mature menopause. You cannot have a child or further children after this procedure. It is a permanent solution to all symptoms caused by fibroids; whether being the best option or not is debatable from the woman's perspective. | |
Sources
Aymara Mas, Marta Tarazona, Joana Dasí Carrasco, Gloria Estaca, Ignacio Cristóbal and Javier Monleón. Updated approaches for management of uterine fibroids. Int J Womens Health. 2017; 9: 607–617.
Last updated on Monday 1 February 2021 11:57 am.
Dowload Product Info Leaflets
Medroxyprogesterone TabletTranexamic Acid Tablet
Ulipristal Acetate Tablet
Levonorgestrel Coil (IUD)
Goserelin Injection
Triporelin Injection